The biopsychosocial model of pain
Understanding the complexity of pain
Pain is a universal experience that affects millions of people around the world. Whether it is a simple headache or a disabling chronic condition, pain can appear in many different ways and have a significant impact on the quality of life of those who experience it.
To better understand this complex experience, some healthcare professionals have adopted the biopsychosocial model of pain, which offers a more global approach adapted to each patient’s reality.
Defining pain
The official IASP definition
According to the International Association for the Study of Pain, IASP, pain is defined as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.”
In this updated 2020 definition, several key aspects are important:
- Sensory and emotional experience: pain is not only a physical sensation. It also involves emotional aspects such as fear, anxiety or distress.
- Unpleasant: pain is perceived as something aversive or uncomfortable, often associated with suffering.
- Actual or potential tissue damage: pain may be due to actual damage, such as an injury or disease, but it can also be experienced without physical damage being present.
This definition therefore recognizes the complexity of pain as a subjective and multidimensional phenomenon, and is widely accepted in the medical and scientific community as a framework for understanding and assessing the pain experience.
The multidimensional nature of pain
The IASP also adds an essential observation:
“Pain is always a personal experience that is influenced to varying degrees by biological, psychological and social factors.”
This statement forms the basis of the biopsychosocial model.
What is the biopsychosocial model of pain?
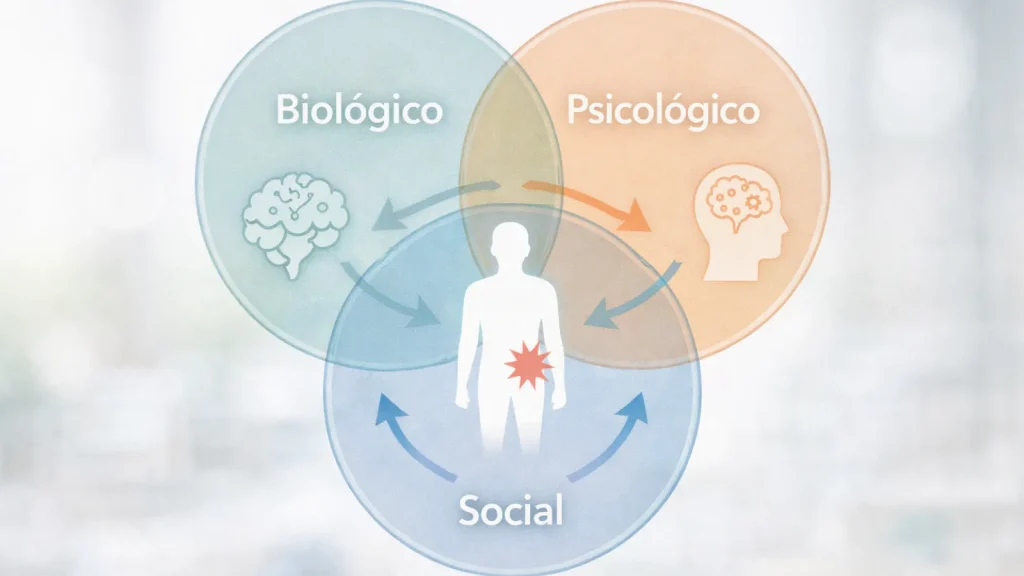
The biopsychosocial model is a comprehensive approach that recognizes that pain is not simply a physical response to an injury or disease. It is the result of the interaction between a person’s biological, psychological and social dimensions.
This approach contrasts with the traditional biomedical model, which tends to focus exclusively on organic aspects and interpret symptoms as direct indicators of disease, without considering the individual’s broader context.
The three dimensions of the biopsychosocial model of pain
Biological dimension
The biological dimension focuses on the physiological, neurobiological and genetic processes involved in pain. It includes the activity of the central and peripheral nervous systems, as well as the mechanisms of transmission and perception.
Understanding the biology of pain is essential for developing effective treatments, although it is not sufficient on its own.
Psychological dimension
The psychological dimension recognizes the influence of emotional and cognitive factors on the pain experience. Anxiety, depression, stress and personal beliefs can modulate pain perception and affect the way people cope with it.
Psychotherapy, cognitive behavioural therapy, CBT, and other psychological interventions can be very helpful in addressing these aspects and helping the patient regain control over their wellbeing.
Social dimension
Finally, the social dimension considers the impact of the environment: family, culture, work, social support, economic situation and access to healthcare. All these factors influence how pain is perceived and managed.
Including the family and community in the therapeutic process can improve outcomes and the patient’s overall quality of life.
Clinical implications
Adopting the biopsychosocial model in clinical practice has profound implications. Healthcare professionals must assess and treat not only the physical aspects of pain, but also its emotional, cognitive and social dimensions.
This requires a multidisciplinary approach involving doctors, psychologists, physiotherapists, osteopaths, social workers and other healthcare professionals.
Practical example: Flora’s story
Onset of pain
Let us take the case of Flora, a young florist. She urgently visits her osteopath because, that same morning, while bending down to pick up a fallen toothbrush, she felt a sharp pain in her lower back. The pain left her immobilized on the floor for almost an hour before she was able to get up with difficulty.
Since then, she has been unable to stand and cannot find any position that relieves her. She is distressed because her father took more than a year to recover from surgery for a lumbar disc herniation. Flora cannot afford to be inactive for that long: she has just opened her business with a bank loan and already feels significant financial pressure.
This is not the first time something similar has happened to her. The last episode was more than a year ago, and the imaging tests performed at the time showed nothing significant.
The role of psychosocial factors
Can we really think that Flora seriously injured herself simply by bending down to pick up an object as light as a toothbrush?
A medical diagnosis is essential, but in most cases — 90% of chronic low back pain is considered non-specific — pain is not due to an inflammatory, traumatic, tumoral or infectious cause.
So why is the pain so intense this time?
Because in the context of low back pain, psychosocial factors are often better predictors of chronicity than biological factors.
Flora has several risk factors:
- stress related to opening her business,
- financial anxiety,
- accumulated fatigue,
- lack of physical activity,
- fear that she has inherited a “fragile back” like her father’s.
Her alarm system is on high alert. A harmless movement is interpreted as a threat, and the brain responds with intense pain.
Neurophysiological mechanisms
What attitude should the therapist adopt?
Back pain is often interpreted as a structural weakness, which generates fear of movement and avoidance behaviours. This vicious cycle maintains pain and disability.
If the therapist simply relieves pain from a purely mechanical approach, for example by relaxing the muscles, and reinforces the idea of a “fragile back”, the risk of relapse increases.
In contrast, a truly effective approach should be based on several pillars:
- pain education, to understand the real mechanisms,
- questioning limiting beliefs,
- gradual re-exposure to movement,
- multidisciplinary treatment that integrates psychological and social dimensions.
In this way, the patient can gradually move out of the pain cycle and regain confidence in their body.
Conclusion: a global and human approach
The biopsychosocial model of pain offers a holistic vision that recognizes the complexity of the pain experience.
By transforming the patient-therapist relationship into an active collaboration, this approach promotes more personalized and effective treatment. Each person is considered as a whole — their beliefs, emotions, history and environment — in order to provide truly patient-centred care.
At Aliantis, this approach is an essential part of our practice. We believe that, to relieve pain in a lasting way, it is necessary to address all its dimensions: biological, psychological and social.
Recognizing the complexity of pain means giving the patient back their place in their own health process.
FAQ about the biopsychosocial model of pain
Does the biopsychosocial model replace traditional medicine?
Which professionals are involved in this approach?
Does it apply only to chronic pain?
This blog article does not aim to generate new knowledge; it is based on the reading of scientific publications, blog articles and other texts.
Sources:
Recursos traducidos de la International Association for the Study of Pain (IASP)
World Health Organization (OMS) – revisión de las directrices sobre el manejo del dolor
Sociedad Española del Dolor (SED) – sección “Psicología y dolor”
Estudio sobre intervención multimodal en dolor crónico
Sociedad Española del Dolor – organización multidisciplinaria sobre el dolor
Plataforma “RetrainPain” en español: enfoque basado en la ciencia para el dolor persistente


